Sacroiliac Joint – the Middle Child
You’ve done a thorough evaluation of the lumbar spine. You’ve done all the special tests for hip pathology, but something is missing. Of course it could be a pelvic floor issue, but what else? Think about the middle child who gets ignored even if making a commotion or goes unnoticed unless being tripped over when standing still. Perhaps the missing link to your patient’s dysfunction is the sacroiliac joint, that “in between” area. If you are unsure how to assess and deal with the “middle child,” learning more about Sacroiliac Joint and Evaluation is something to add to your professional bucket list.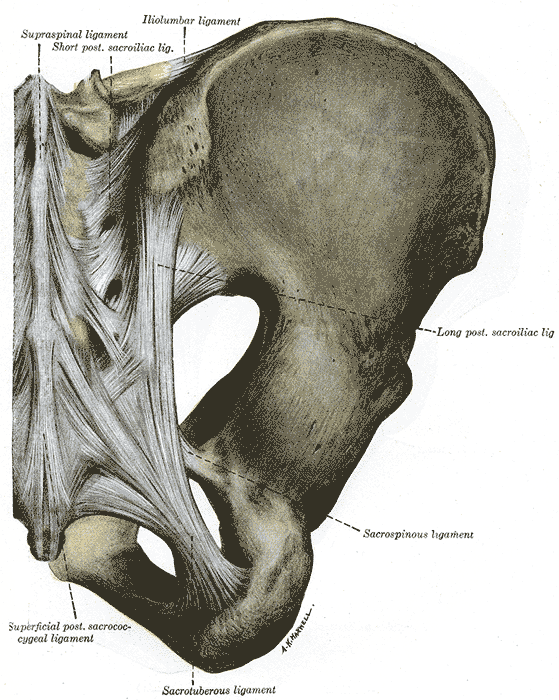
According to the special tests book by Chad Cook, a pain mapping test suggests a referral pattern of SI dysfunction as pain in the buttock unilaterally, below the level of L5, without symptoms in the midline. Often we are on a mission to make the lumbar spine the source of symptoms, but this provides some guideline as to where the pain would be located if the SI joint were the guilty party. If pain is found above L5, the SI joint is likely not the primary tissue in lesion. If the pain is bilateral, the issue is more than just SI joint.(Cook, 2013)
The special tests to diagnose SI joint dysfunction have been considered in a cluster. According to Laslett, distraction, compression, thigh thrust, Gaenslens, and Patricks are the primary tests used to assess SI dysfunction. Three or more of these tests being positive can help a clinician rule in SI joint as a diagnosis, with SI joint blocks being just as predictive. When pain cannot be centralized, and three of the tests are positive, there is a 77% probability the SI joint is the source of pain; and, in the pregnant population, there is an 89% chance the SI joint is the culprit of pain.(Laslett, 2008)
While parents keep up with the oldest and youngest, the middle child can be hard at work causing dysfunction that disrupts the whole family. Likewise, the sacroiliac joint can be hypermobile, hypomobile or have ligamentous strain, yet we therapists may ignore any signs until the lumbar spine or hip or pelvic floor are suddenly provocative. The longer an SI joint dysfunction goes undiagnosed and untreated, the greater the likelihood of pelvic floor dysfunction, secondary to its intimate relationship to the area. A catawampus ilium position on the sacrum can cause hip pain, and the ilium’s relationship to the sacrum can aggravate the lumbar spine. We just need to use all our diagnostic tools to discern what is making our patients symptomatic and then prioritize the treatment.
Taking the upcoming sacroiliac course through Herman Wallace (Sep. 12-13 in New Orleans) will make the “middle child” become respected, understood, and never left wanting again. Review the anatomy, explore and proficiently perform the special tests, and effectively implement treatment and stabilization of the SI joint during this course. You owe your patients the ability to understand the lumbar region and pelvic ring in their entirety and leave no source of pain a mystery.
References:
Cook, C., & Hegedus, E. (2013). Orthopedic physical examination tests: An evidence-based approach. Upper Saddle River, N.J.: PearsonPrentice Hall.
Laslett, M. (2008). Evidence-Based Diagnosis and Treatment of the Painful Sacroiliac Joint. The Journal of Manual & Manipulative Therapy, 16(3), 142–152.
By accepting you will be accessing a service provided by a third-party external to https://hermanwallace.com./
All Upcoming Continuing Education Courses

Parkinson Disease and Pelvic Rehabilitation - Remote Course - April 25 - 26 2025
Apr 25 2025 - Apr 26 2025

Pelvic Function Level 1 - Satellite - New York NY - April 26 - 27 2025 - SOLD OUT
Apr 26 2025 - Apr 27 2025

Menopause Transitions and Pelvic Rehab - Remote Course - April 26 - 27 2025
Apr 26 2025 - Apr 27 2025



Pediatrics Level 1 - Treatment of Bowel and Bladder Disorders - Remote Course - April 26 - 27 2025 - SOLD OUT
Apr 26 2025 - Apr 27 2025




Pelvic Function Level 1 - Satellite - Colorado Springs CO - April 26 - 27 2025 - SOLD OUT
Apr 26 2025 - Apr 27 2025







Biofeedback for Pelvic Muscle Dysfunction Satellite Lab Course - Self-Hosted - May 4 2025
May 4 2025





Pelvic Function Level 1 - Satellite - Plainfield IN - May 10 - 11 2025 - SOLD OUT
May 10 2025 - May 11 2025





Pelvic Function Level 1 - Satellite - Las Vegas NV - May 10 - 11 2025 - SOLD OUT
May 10 2025 - May 11 2025

Mobilization of Visceral Fascia: The Urinary System Satellite Lab Course - Bradenton FL - May 16 - 18 2025
May 16 2025 - May 18 2025

Mobilization of Visceral Fascia: The Urinary System Satellite Lab Course - Philadelphia PA - May 16 - 18 2025
May 16 2025 - May 18 2025

Mobilization of Visceral Fascia: The Urinary System Satellite Lab Course - Atlanta GA - May 16 - 18 2025 (Instructor Site)
May 16 2025 - May 18 2025
Mobilization of Visceral Fascia: The Urinary System Satellite Lab Course - Self-Hosted - May 16 - 18 2025
May 16 2025 - May 18 2025

Mobilization of Visceral Fascia: The Urinary System Satellite Lab Course - Bellingham WA - May 16 - 18 2025
May 16 2025 - May 18 2025





Lumbar Nerve Manual Assessment and Treatment - Remote Course - May 17 - 18 2025
May 17 2025 - May 18 2025



Pelvic Function Level 1 - Satellite - Galloway NJ - May 31 - June 1 2025 - SOLD OUT
May 31 2025 - Jun 1 2025
