Often pelvic floor therapists see men for post-prostatectomy urinary leakage. However, at least for me, that quickly led to seeing male patients for pelvic pain and sexual dysfunction. Male sexual dysfunction is a broad category and can consist of erectile dysfunction (ED), ejaculation disorders including premature ejaculation (PE), and low libido -- often there is a pelvic floor muscle (PFM) dysfunction component. Conservative treatment frequently consists of pharmacological and lifestyle changes for this population.
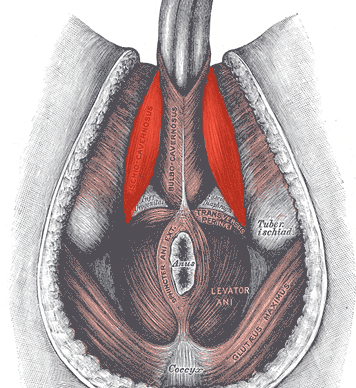
In normal sexual function, the male superficial pelvic floor musculature (bulbocavernosus and ischiocavernosus) work together to create increased intracavernosus pressure by limiting venous return, resulting in an erection. Ejaculation is created by rhythmic contractions of the bulbocavernosus muscle.
 The authors of this systematic review were curious if pelvic floor muscle training was effective for treating erectile dysfunction and premature ejaculation diagnoses, and if so to determine whether there is a treatment protocol. Ten studies were found that met the inclusion criteria, five that focused on ED and five that focused on PE. In total, there were 668 participants ranging in age from 30-59 years old. Studies were excluded if participants were post-prostatectomy and/or had a neurological diagnosis. The intervention was a pelvic floor program, and pelvic floor muscle contractions were either taught or supervised. Studies also included supportive treatment including biofeedback, lifestyle changes, and electrical stimulation.
The authors of this systematic review were curious if pelvic floor muscle training was effective for treating erectile dysfunction and premature ejaculation diagnoses, and if so to determine whether there is a treatment protocol. Ten studies were found that met the inclusion criteria, five that focused on ED and five that focused on PE. In total, there were 668 participants ranging in age from 30-59 years old. Studies were excluded if participants were post-prostatectomy and/or had a neurological diagnosis. The intervention was a pelvic floor program, and pelvic floor muscle contractions were either taught or supervised. Studies also included supportive treatment including biofeedback, lifestyle changes, and electrical stimulation.
The studies focused on erectile dysfunction listed a combination of hormonal, psychogenic, arteriogenic, and venogenic causes. The pelvic floor training ranged from 5-20 visits over 3-4 months and included a home exercise program. Pelvic floor training was similar in all studies and consisted of maximal quick contractions over one second and submaximal endurance holds over 6-10 seconds. Compliance to home exercise program was not assessed. Between 35% and 47% of participants reported a full resolution of symptoms. Subjective improvements were supported by improved maximal anal pressure and intracavernosus pressure. One study used the International Index of Erectile Function (IIEF) and showed significant improvement (p<0.05).
The studies focused on premature ejaculation noted participants had either lifelong or secondary PE. The pelvic floor training in these studies ranged from 12-20 sessions over 1-3 months. All studies used electrical stimulation as part of the pelvic floor muscle training. Four studies also used biofeedback. Only one study listed a home exercise program but did not report on compliance. The pelvic floor muscle training was compared to nothing in three studies, and to a selective serotonin reuptake inhibitor (SSRI) in the other two studies. Patient reported full resolution of symptoms was 55-83% in two studies, and there was a significant improvement in delay in heterosexual penetrative ejaculation (p<0.05) in three studies.
For both erectile dysfunction and premature ejaculation, pelvic floor muscle exercise prescription was 2-3 times per week with pelvic floor muscle contractions both maximal quick contractions and submaximal endurance holds. Significant results were shown with participants who were taught pelvic floor muscle contractions through a combination of verbal and physical means (typically biofeedback). Specific verbal cues were not reported. The authors suggest that electrical stimulation was helpful for training recruitment patterns; however, there was not a significant difference in outcomes for those with ED when using electrical stimulation. The authors suggest that pelvic floor muscle training can be part of a conservative treatment. It may be used with oral pharmacology for quick results, and may be beneficial with electrical stimulation and biofeedback, though more research is indicated.
If you are interested in learning more about treating male patients, consider attending Male Pelvic Floor: Function, Dysfunction, and Treatment!
Myers, C., Smith, M. “Pelvic floor muscle training improves erectile dysfunction and premature ejaculation: a systematic review” Physiotherapy 105 (2019) 235–243
All Upcoming Continuing Education Courses

Pelvic Function Level 1 - Satellite - New York NY - April 26 - 27 2025 - SOLD OUT
Apr 26 2025 - Apr 27 2025

Menopause Transitions and Pelvic Rehab - Remote Course - April 26 - 27 2025
Apr 26 2025 - Apr 27 2025

Pelvic Function Level 1 - Satellite - Bethpage NY - April 26 - 27 2025 - SOLD OUT
Apr 26 2025 - Apr 27 2025

Pediatrics Level 1 - Treatment of Bowel and Bladder Disorders - Remote Course - April 26 - 27 2025 - SOLD OUT
Apr 26 2025 - Apr 27 2025




Pelvic Function Level 1 - Satellite - Colorado Springs CO - April 26 - 27 2025 - SOLD OUT
Apr 26 2025 - Apr 27 2025

Pelvic Function Level 1 - Satellite - Marietta GA - April 26 - 27 2025 - SOLD OUT
Apr 26 2025 - Apr 27 2025






Biofeedback for Pelvic Muscle Dysfunction Satellite Lab Course - Self-Hosted - May 4 2025
May 4 2025





Pelvic Function Level 1 - Satellite - Plainfield IN - May 10 - 11 2025 - SOLD OUT
May 10 2025 - May 11 2025





Pelvic Function Level 1 - Satellite - Las Vegas NV - May 10 - 11 2025 - SOLD OUT
May 10 2025 - May 11 2025

Mobilization of Visceral Fascia: The Urinary System Satellite Lab Course - Bradenton FL - May 16 - 18 2025
May 16 2025 - May 18 2025

Mobilization of Visceral Fascia: The Urinary System Satellite Lab Course - Philadelphia PA - May 16 - 18 2025
May 16 2025 - May 18 2025

Mobilization of Visceral Fascia: The Urinary System Satellite Lab Course - Atlanta GA - May 16 - 18 2025 (Instructor Site)
May 16 2025 - May 18 2025
Mobilization of Visceral Fascia: The Urinary System Satellite Lab Course - Self-Hosted - May 16 - 18 2025
May 16 2025 - May 18 2025

Mobilization of Visceral Fascia: The Urinary System Satellite Lab Course - Bellingham WA - May 16 - 18 2025
May 16 2025 - May 18 2025





Lumbar Nerve Manual Assessment and Treatment - Remote Course - May 17 - 18 2025
May 17 2025 - May 18 2025



Pelvic Function Level 1 - Satellite - Galloway NJ - May 31 - June 1 2025 - SOLD OUT
May 31 2025 - Jun 1 2025


Pediatrics Level 2 - Adv Pediatric Bowel and Bladder Disorders - Remote Course - May 31 - Jun 1 2025
May 31 2025 - Jun 1 2025
