This week Ramona Horton sat down with Holly Tanner to discuss manual therapy and her course Mobilization of the Myofascial Layer: Pelvis and Lower Extremity. The following is an excerpt from her interview.
What do we really know about manual therapy? We have decent evidence that shows that asymmetry matters. The tenet of the myofascial course is an osteopathic tenet called ARTS:
- Asymmetry
- Restriction of Mobility
- Tissue Texture Changes
- Sensitivity
The whole myofascial course is designed around looking for ARTS. When you find the asymmetry within the myofascial system then that’s where you direct your efforts and energy.
Often patients have already tried breathing, yoga, medication, etcetera – and it’s the manual therapy piece that they often have not had. It’s not that uncommon for me to be someone’s second or third therapist. Some patients may have tried some type of manual therapy but it was more things like ischemic compression where the problem was that the manual therapy was triggering nociception.
So in the myofascial course, we start with ARTS but we also have an idea where we flip ARTS on its head and we go to STAR. In STAR, you take sensitivity and put it at the top of your list. That becomes the highest portion in your paradigm. Then we use simple techniques that are not non-nociceptive. Indirect technique versus direct technique, such as something as simple as positional inhibition.
The whole idea of the myofascial course is to teach people to think and problem solve. Then have a very broad spectrum way of you find an inner articular issue where this joint is moving and this one is not. Learn to not chase the booboo. Just because it hurts on the right doesn’t mean that you’re going to treat the right. It might hurt on the right because there is a hypo-mobility on the left. Let’s treat where the brain is protecting the tissue, and holding, and guarding the tissue. Trust in the belief that the body is a self-righting mechanism. The body will then normalize itself.
In manual therapy, our job is to get the body moving like it's supposed to. It’s not to fix the ‘booboo.’ The issue is not in the tissue. If the tissue is tight, it’s tight because the brain is keeping it that way. The way I teach manual therapy is the fascial system gives us access to the nervous system. By utilizing the fascial system in a non-nociceptive manner, what we’re really doing is just having a conversation with the brain. We’re not fixing the tissue. That’s the whole premise of the course - to get people to understand and change their thinking and their paradigm to ask what the brain is protecting and utilizing the fascial system.

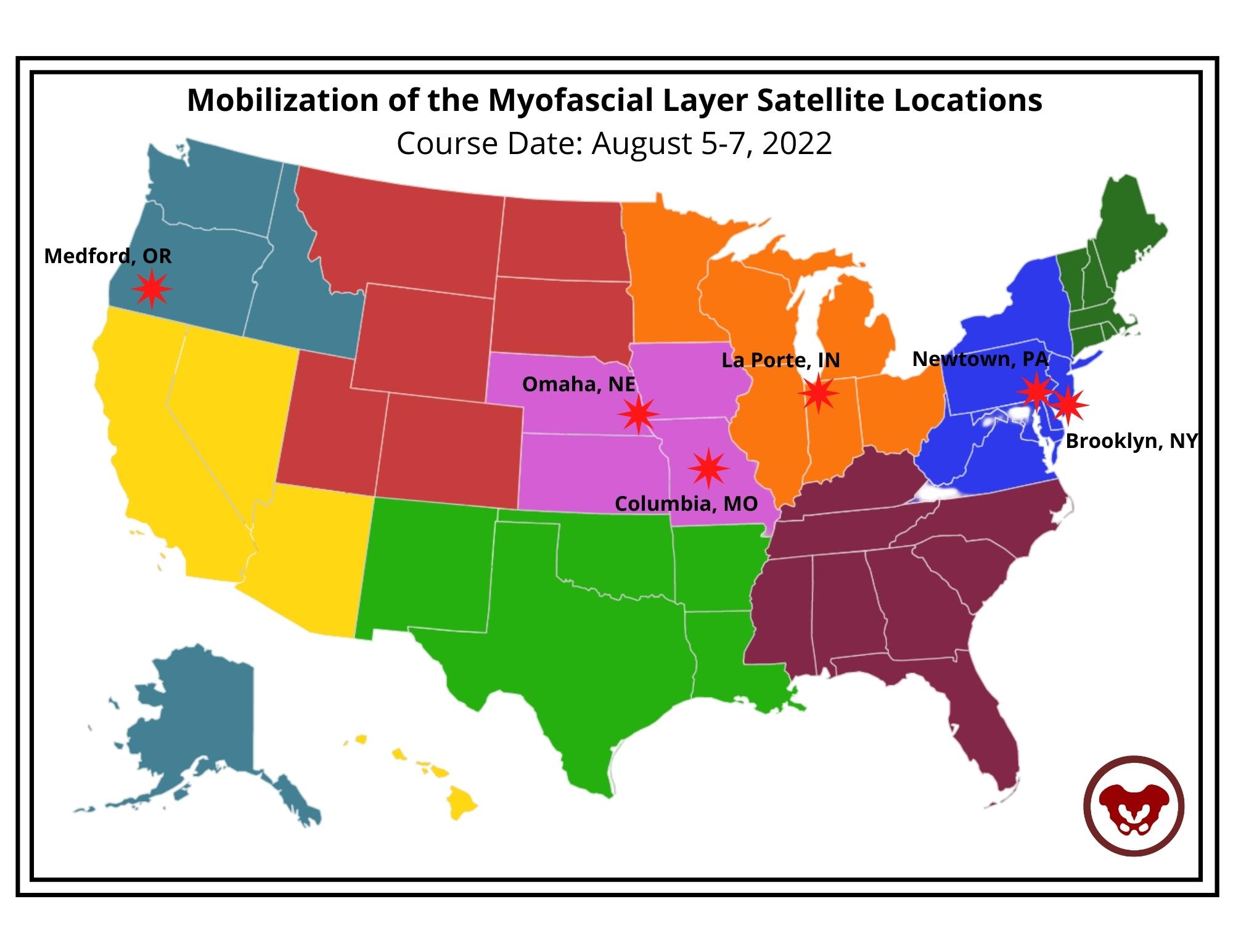
Course Date: August 5-7, 2022
- Self-Hosted - for groups of at least 2 qualified practitioners.

Manual Therapy for the Abdominal Wall allows practitioners to review how everything interplays within the myofascial system and apply specific techniques. These techniques include how to assess the tissue for mobility, how to treat tissues that are restricted in the abdominal wall, and how to treat scar tissue. How do we help somebody who can’t lay flat because their abdominal wall has become restricted for so long because of possible pain? Possibly due to surgery. Possibly due to fear. How do we help those patients get back to function?
Over the past 10 plus years of teaching the pelvic series with Herman & Wallace, Tina Allen noticed that for some of the participants there was a gap in confidence in palpation skills and treatment techniques applied to the pelvic floor region. For most, it’s confidence in where they are and what they are feeling on the patient. Manual Therapy for the Abdominal Wall came out of wanting to fill that gap. This course is really about taking some of those skills and then applying them to the abdominal wall.
Abdominal pain can arise from many origins including abdominal scars, endometriosis, IC/PBS, and abdominal wall restrictions that impact pelvic girdle dysfunction. An older study, back in 2007 by Geoff Harding focused on back, chest, and abdominal pain and whether it was spinal referred pain and employed manual therapy as part of his treatments for his case studies. Harding found that “More specific treatment of the origin of the pain may then include manual therapy, including mobilization (gentle rhythmic movement), … applied to the affected segment can be very effective in reducing movement restriction – and pain. These simple treatments were used in all three case studies to good effect.” (1)
This research was supported by Rice et al. in 2013 when their research on non-surgical treatment of adhesion-related small bowel obstructions showed that “those patients who underwent the manual therapy demonstrated increased range of motion … and an early return to normal activities of daily living simply enhanced the benefits.” (2) Manual therapy has no recovery time and allows patients to recover and participate in daily activities while promoting the return of normal tissue function, range of motion, and increased blood flow.
Tina Allen explains that manual therapy is about “asking for permission to touch and using our hands to help the patient integrate into their system again. The patient may not realize that they’ve been holding, that there is tension or rigidity in the tissues.” Tina continues to share that “for me, manual therapy fits in to help folks realize, or feel, what’s happening in their body again. And then allowing them to make that change. I use manual therapy to allow a patient to move better. To become more aware in their body.” The full interview with Tina can be viewed below or on the Herman & Wallace YouTube Channel.
Manual Therapy for the Abdominal Wall is a beginner-level class and is filled with practitioners just beginning their pelvic floor journey through experienced clinicians taking the course to learn something new. The techniques instructed by Tina Allen are immediately applicable in the clinic. Course dates for 2022 include:
References:
- Harding G, Yelland M (2007). Back, chest, and abdominal pain. Australian Family Physician, 36(6), 422-429.
- Rice, A. D., King, R., Reed, E. D., Patterson, K., Wurn, B. F., & Wurn, L. J. (2013). Manual Physical Therapy for Non-Surgical Treatment of Adhesion-Related Small Bowel Obstructions: Two Case Reports. Journal of clinical medicine, 2(1), 1–12.
All Upcoming Continuing Education Courses

Parkinson Disease and Pelvic Rehabilitation - Remote Course - April 25 - 26 2025
Apr 25 2025 - Apr 26 2025

Pelvic Function Level 1 - Satellite - New York NY - April 26 - 27 2025 - SOLD OUT
Apr 26 2025 - Apr 27 2025

Menopause Transitions and Pelvic Rehab - Remote Course - April 26 - 27 2025
Apr 26 2025 - Apr 27 2025



Pediatrics Level 1 - Treatment of Bowel and Bladder Disorders - Remote Course - April 26 - 27 2025 - SOLD OUT
Apr 26 2025 - Apr 27 2025




Pelvic Function Level 1 - Satellite - Colorado Springs CO - April 26 - 27 2025 - SOLD OUT
Apr 26 2025 - Apr 27 2025







Biofeedback for Pelvic Muscle Dysfunction Satellite Lab Course - Self-Hosted - May 4 2025
May 4 2025





Pelvic Function Level 1 - Satellite - Plainfield IN - May 10 - 11 2025 - SOLD OUT
May 10 2025 - May 11 2025





Pelvic Function Level 1 - Satellite - Las Vegas NV - May 10 - 11 2025 - SOLD OUT
May 10 2025 - May 11 2025

Mobilization of Visceral Fascia: The Urinary System Satellite Lab Course - Bradenton FL - May 16 - 18 2025
May 16 2025 - May 18 2025

Mobilization of Visceral Fascia: The Urinary System Satellite Lab Course - Philadelphia PA - May 16 - 18 2025
May 16 2025 - May 18 2025

Mobilization of Visceral Fascia: The Urinary System Satellite Lab Course - Atlanta GA - May 16 - 18 2025 (Instructor Site)
May 16 2025 - May 18 2025
Mobilization of Visceral Fascia: The Urinary System Satellite Lab Course - Self-Hosted - May 16 - 18 2025
May 16 2025 - May 18 2025

Mobilization of Visceral Fascia: The Urinary System Satellite Lab Course - Bellingham WA - May 16 - 18 2025
May 16 2025 - May 18 2025





Lumbar Nerve Manual Assessment and Treatment - Remote Course - May 17 - 18 2025
May 17 2025 - May 18 2025



Pelvic Function Level 1 - Satellite - Galloway NJ - May 31 - June 1 2025 - SOLD OUT
May 31 2025 - Jun 1 2025
