
Did you know that Ramona Horton is going to be speaking at HWConnect in March? Her lecture is titled, “The Do Not Miss List: What many pelvic rehab therapists overlook." I don’t know about you, but we’re pretty excited to hear what she has to say and to learn from the best!
So, who is Ramona C. Horton MPT, DPT?
Ramona completed her graduate training in the US Army–Baylor University Program in Physical Therapy in San Antonio, TX. She exited the army at the rank of Captain and applied her experience with the military orthopedic population in the civilian sector as she developed a growing interest in the field of pelvic dysfunction and received her post-professional Doctorate in Physical Therapy from A.T. Still University in Mesa, AZ. In 2020, Ramona received the prestigious Academy of Pelvic Health Elizabeth Noble Award for her contributions to the field of pelvic health.
Ramona is the lead therapist for her clinic's pelvic dysfunction program in Medford, OR where her practice focuses on the treatment of urological, gynecological, and colorectal issues. Ramona has completed advanced studies in manual therapy with an emphasis on spinal manipulation, and visceral and fascial mobilization.
Not only is Ramona Horton, MPT, DPT speaking at HWConnect 2025 in March, but she has also developed and instructs the Visceral and Fascial Mobilization Course Series for Herman & Wallace. If you haven’t taken a course from Ramona or heard her speak, then we highly recommend that you do!
The top 3 reasons to sign up for a course with Ramona Horton are:
1. Understand the true function and mechanisms of manual therapy.
Manual therapy is presented as a concept and technique that does NOT “release” tight or bound fascia based on the skill or magic hands of the practitioner. The issue is not in the tissue, if the tissue is tight, it’s tight because the brain is keeping it that way. Muscles are marionettes, and the brain is the puppet master. Manual therapy utilizes the fascial system to access the nervous system. In other words, having a conversation with the brain over the tissue that it appears to be protecting while trusting that the homeostatic mechanism is functioning in the body. If this is done in a non-threatening manner, the brain will normalize the tissue it is holding and guarding.
2. Add a whole host of new tools to your practitioner toolbelt.
The myofascial course teaches basic screening techniques that will point you in the right direction toward finding where the body is protecting, not where symptoms are being expressed. You will learn a variety of techniques to approach different fascial layers including direct and indirect fascial stacking for superficial nerves within the panniculus, muscular, and articular restrictions, as well as indirect technique of positional inhibition for trigger points. In addition, the science behind basic neural mobilization, instrument-assisted fascial mobilization, and fascial decompression (cupping) are presented.
3. Learn more about fascia, its origins, and its functions.
Fascia is EVERYWHERE throughout the body; it is the ubiquitous connective tissue that holds every cell together much like the mortar in a brick wall, in addition to cells, it connects every system in the body. Fascia contains a vast neurological network including nociceptors, mechanoreceptors, and proprioceptors just to name a few. The fascial system has multiple layers within the body: starting at the panniculus which blends with the skin, the investing fascia surrounding muscles and forming septae, the visceral fascia which is by far the most complex and the deepest layer of fascia, the dura surrounding the central nervous system extending to the peripheral nerves. All fascial structures, regardless of layer or location have their origin in the mesoderm of early embryologic development. The myofascial course presents evaluation and treatment techniques for three of the four fascial layers while the three visceral courses address the complex visceral fascial layer.
Ramona Horton's Mobilization Series 2024 Course Schedule
The Mobilization courses are available in satellite and self-hosted formats. PLUS Ramona is going on the road this year and will be teaching directly from different satellites for each course. Find out more on the Visceral and Fascial Mobilization Course Series home page. Satellite locations can be found on the main course page and may change, be added or removed, for future course events.
Mobilization of the Myofascial Layer: Pelvis and Lower Extremity - Satellite Lab Course
April 4-6
Bradenton FL
Medford OR
Milwaukee WI
Novato CA
St. Petersburg FL
Torrance CA
Self-Hosted
Mobilization of Visceral Fascia: The Gastrointestinal System - Satellite Lab Course
March 7-9
Appleton WI
Lansing MI
Nashville TN
Portland ME
Tampa FL
Torrance CA
Tuscon AZ
Self-Hosted
June 27-29
Milwaukee WI
St. Petersburg FL
Sellersville PA
Self-Hosted
Mobilization of Visceral Fascia: The Urinary System - Satellite Lab Course
January 31-February 2
Fort Lauderdale FL
Medford OR
Tampa FL
Torrance CA
Wichita KS
Self-Hosted
May 16-18
Atlanta GA
Bradenton FL
Philadelphia PA
Self-Hosted
November 14-16
Milwaukee WI
Stevens Point WI
Self-Hosted
Mobilization of Visceral Fascia: The Reproductive System - Satellite Lab Course
October 17-19
Milwaukee WI
Omaha NE
Torrance CA
Tuscon AZ
Self-Hosted
This week Ramona Horton sat down with Holly Tanner to discuss manual therapy and her course Mobilization of the Myofascial Layer: Pelvis and Lower Extremity. The following is an excerpt from her interview.
What do we really know about manual therapy? We have decent evidence that shows that asymmetry matters. The tenet of the myofascial course is an osteopathic tenet called ARTS:
- Asymmetry
- Restriction of Mobility
- Tissue Texture Changes
- Sensitivity
The whole myofascial course is designed around looking for ARTS. When you find the asymmetry within the myofascial system then that’s where you direct your efforts and energy.
Often patients have already tried breathing, yoga, medication, etcetera – and it’s the manual therapy piece that they often have not had. It’s not that uncommon for me to be someone’s second or third therapist. Some patients may have tried some type of manual therapy but it was more things like ischemic compression where the problem was that the manual therapy was triggering nociception.
So in the myofascial course, we start with ARTS but we also have an idea where we flip ARTS on its head and we go to STAR. In STAR, you take sensitivity and put it at the top of your list. That becomes the highest portion in your paradigm. Then we use simple techniques that are not non-nociceptive. Indirect technique versus direct technique, such as something as simple as positional inhibition.
The whole idea of the myofascial course is to teach people to think and problem solve. Then have a very broad spectrum way of you find an inner articular issue where this joint is moving and this one is not. Learn to not chase the booboo. Just because it hurts on the right doesn’t mean that you’re going to treat the right. It might hurt on the right because there is a hypo-mobility on the left. Let’s treat where the brain is protecting the tissue, and holding, and guarding the tissue. Trust in the belief that the body is a self-righting mechanism. The body will then normalize itself.
In manual therapy, our job is to get the body moving like it's supposed to. It’s not to fix the ‘booboo.’ The issue is not in the tissue. If the tissue is tight, it’s tight because the brain is keeping it that way. The way I teach manual therapy is the fascial system gives us access to the nervous system. By utilizing the fascial system in a non-nociceptive manner, what we’re really doing is just having a conversation with the brain. We’re not fixing the tissue. That’s the whole premise of the course - to get people to understand and change their thinking and their paradigm to ask what the brain is protecting and utilizing the fascial system.

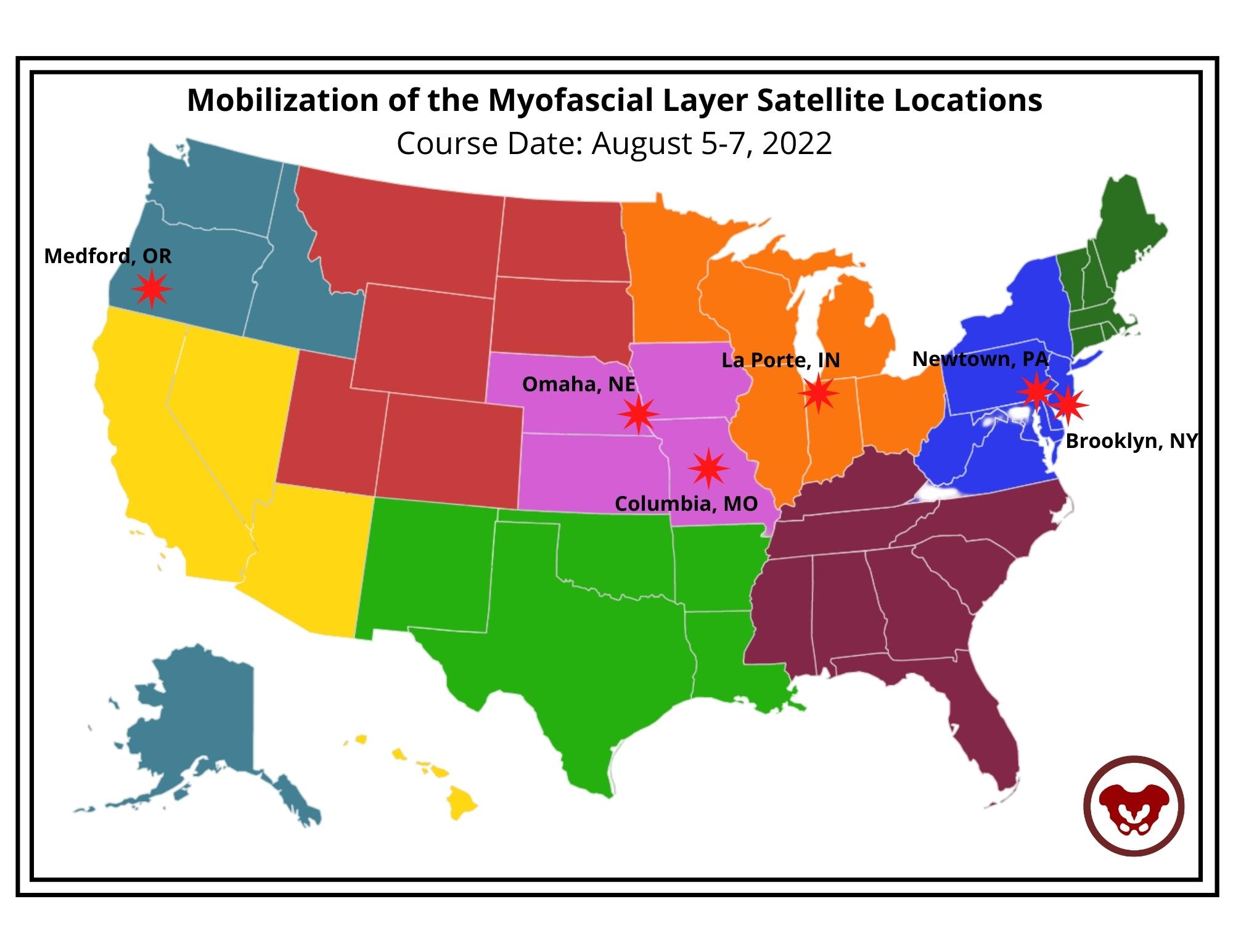
Course Date: August 5-7, 2022
- Self-Hosted - for groups of at least 2 qualified practitioners.


This blog includes portions of an interview with Ramona Horton. Ramona serves as the lead therapist for her clinic's pelvic dysfunction program in Medford, OR. Her practice focuses on patients with urological, gynecological, and colorectal issues. Ramona has completed advanced studies in manual therapy with an emphasis on spinal manipulation, and visceral and fascial mobilization. She developed and instructs her visceral and fascial mobilization courses for the Herman & Wallace Pelvic Rehabilitation Institute, and presents frequently at local, national, and international venues on topics relating to women’s health, pelvic floor dysfunction, and manual therapy.
How did you start in pelvic rehabilitation and visceral mobilization?
My PT training was through the Army-Baylor program, I was all in for orthopedics and sports medicine until October of 1990. I gave birth to my second child, an adorable, but behemoth, 9lb 9oz baby boy. His delivery, a VBAC (vaginal birth after cesarean) was very traumatic on my pelvis, I sustained pudendal nerve injury and muscular avulsion. When I queried the attending OB-GYN about my complete lack of bladder control his response and I quote “do a thousand Kegels a day, and when you’re 40 and want a hysterectomy, we’ll fix your bladder then.” As for the desire to study visceral mobilization, that reflects back to my PT training through the US Army which was 30 years ago, when the MPT was just getting started. It was an accelerated program, to say the least. We received a master's in physical therapy with 15 months of schooling. Given the very limited timeline, which included affiliations and thesis, the emphasis in our training was on critical thinking and problem solving, not memorization and protocols which in 1985 was not the norm. I can still hear the words of our instructors “You have to figure it out, I am not going to give you a cookbook."
Following my initial training in the field of pelvic dysfunction in 1993 I started treating patients. I had a problem, I could not wrap my head around how I was to effectively treat bowel and bladder dysfunction…. without treating the bowel and bladder? I knew that there was more to this anatomy than just pelvic floor muscles and the abdominal wall, but at the time that is what was being treated. Once I started learning VM principles and applying the techniques to my patients I saw a vast improvement in my outcomes. I realized that the visceral fascia is a huge missing link in this field and that somewhere along the line the physical therapy community forgot one simple fact. We are not hollow; the visceral structures attach to the somatic frame through ligaments and connective tissue and have an influence on the biomechanics of said frame.
Why is the adoption of visceral mobilization so rare amongst practitioners who aren’t pelvic specialists?
Most likely several reasons, first they do not deal with dysfunctions that have visceral structures involved the way pelvic health therapists do. The second is a paucity of higher levels of evidence on the effectiveness of VM for musculoskeletal conditions. The third and most difficult issue to deal with is the broad-based claims that VM can be an effective treatment for issues ranging from acute trauma to emotional problems. One website called VM “bloodless surgery”. The problem simply is when anyone purports their technique to be a virtual panacea for all that ails mankind, without adequate evidence to back up the claims, the clinical world raises its collective antennae. These critical remarks are coming from a practitioner, published author, and educator in the VM field. The reality of evidence-based medicine is talk is cheap, research is not.
Why do you believe fascial mobilization is such an important aspect of clinical practice?
Most importantly because fascia is ubiquitous, it is EVERYWHERE throughout the body and it contains a vast neurological network to include nociceptors, mechanoreceptors, and proprioceptors just to name a few. The fascia was that stuff that we all dissected out of the way in anatomy lab so we could learn the assigned structures that soon would have a pin with a number stuck in it that we needed to know for a lab practical. We need to move beyond the “myofascia” and understand that the fascial system has multiple layers in the body starting at the panniculus which blends with the skin, the investing fascia surrounding muscles and forming septae, the visceral fascia which is by far the most complex and the deepest layer of fascia, the dura surrounding the central nervous system. All fascial structures, regardless of layer or location have their origin in the mesoderm of early embryologic development.
Ramona Horton's Fascial Mobilization Series 2022 Course Schedule
Mobilization of the Myofascial Layer: Pelvis and Lower Extremity Satellite Lab Course
Mobilization of Visceral Fascia: The Urinary System Satellite Lab Course
Mobilization of Visceral Fascia: The Gastrointestinal System Satellite Lab Course
September 30 - October 2, 2022
Mobilization of Visceral Fascia: The Reproductive System Satellite Lab Course
All Upcoming Continuing Education Courses

Parkinson Disease and Pelvic Rehabilitation - Remote Course - April 25 - 26 2025
Apr 25 2025 - Apr 26 2025

Pelvic Function Level 1 - Satellite - New York NY - April 26 - 27 2025 - SOLD OUT
Apr 26 2025 - Apr 27 2025

Menopause Transitions and Pelvic Rehab - Remote Course - April 26 - 27 2025
Apr 26 2025 - Apr 27 2025



Pediatrics Level 1 - Treatment of Bowel and Bladder Disorders - Remote Course - April 26 - 27 2025 - SOLD OUT
Apr 26 2025 - Apr 27 2025




Pelvic Function Level 1 - Satellite - Colorado Springs CO - April 26 - 27 2025 - SOLD OUT
Apr 26 2025 - Apr 27 2025







Biofeedback for Pelvic Muscle Dysfunction Satellite Lab Course - Self-Hosted - May 4 2025
May 4 2025





Pelvic Function Level 1 - Satellite - Plainfield IN - May 10 - 11 2025 - SOLD OUT
May 10 2025 - May 11 2025





Pelvic Function Level 1 - Satellite - Las Vegas NV - May 10 - 11 2025 - SOLD OUT
May 10 2025 - May 11 2025

Mobilization of Visceral Fascia: The Urinary System Satellite Lab Course - Bradenton FL - May 16 - 18 2025
May 16 2025 - May 18 2025

Mobilization of Visceral Fascia: The Urinary System Satellite Lab Course - Philadelphia PA - May 16 - 18 2025
May 16 2025 - May 18 2025

Mobilization of Visceral Fascia: The Urinary System Satellite Lab Course - Atlanta GA - May 16 - 18 2025 (Instructor Site)
May 16 2025 - May 18 2025
Mobilization of Visceral Fascia: The Urinary System Satellite Lab Course - Self-Hosted - May 16 - 18 2025
May 16 2025 - May 18 2025

Mobilization of Visceral Fascia: The Urinary System Satellite Lab Course - Bellingham WA - May 16 - 18 2025
May 16 2025 - May 18 2025





Lumbar Nerve Manual Assessment and Treatment - Remote Course - May 17 - 18 2025
May 17 2025 - May 18 2025



Pelvic Function Level 1 - Satellite - Galloway NJ - May 31 - June 1 2025 - SOLD OUT
May 31 2025 - Jun 1 2025
