
Erica Vitek, MOT, OTR, BCB-PMD, PRPC is the author and presenter of the new Parkinson Disease and Pelvic Rehabilitation course, and she is the co-author of the Neurologic Conditions and Pelvic Floor Rehab course. She is a certified LSVT (Lee Silverman) provider and faculty member, and is a trained PWR! (Parkinson’s Wellness Recovery) provider, both focusing on intensive, amplitude and neuroplasticity based exercise programs for people with Parkinson disease. Erica partners with the Wisconsin Parkinson Association (WPA) as a support group and event presenter as well as author in their publication, The Network. Erica has taken a special interest in the unique pelvic floor, bladder, bowel and sexual health issues experienced by individuals diagnosed with Parkinson disease.
 Parkinson disease is the second most common neurologic disorder. When most people think about people with Parkinson disease, they think about stooped posture, shuffling gait, slow and rigid movement, balance difficulties and tremoring. Often these motor symptoms are the main target of pharmacological treatments with neurologists and many experience positive functional gains. Non-motor symptoms, however, can be more disabling than the motor symptoms and have significant adverse effects on the quality of life in people with Parkinson disease.
Parkinson disease is the second most common neurologic disorder. When most people think about people with Parkinson disease, they think about stooped posture, shuffling gait, slow and rigid movement, balance difficulties and tremoring. Often these motor symptoms are the main target of pharmacological treatments with neurologists and many experience positive functional gains. Non-motor symptoms, however, can be more disabling than the motor symptoms and have significant adverse effects on the quality of life in people with Parkinson disease.
The pharmacologic management of non-motor autonomic dysfunction, including urinary, bowel, and sexual health impairments, is often ineffective, not supported by adequate research, or causes intolerable side effects for people with Parkinson disease. In a recent article titled Update on Treatments for Nonmotor Symptoms of Parkinson’s Disease – An Evidence-Based Medicine Review Seppi, K, et al., 2019, the authors state that “before attempting any [pharmacological] treatment for lower urinary tract symptoms, urinary tract infections, prostate disease in men, and pelvic floor disease in women should be ruled out.” It is rare to see a mention of pelvic floor within the literature that addresses helping people with Parkinson disease.
Pelvic rehabilitation specialists have a unique opportunity to step in and help these individuals improve their quality of life and many neurologists are unaware of the benefits our services could provide for their patients. Please join me in an exciting dive into understanding the physiology of how Parkinson disease affects a person’s pelvic health and develop your skills to effectively assess and develop treatment plans to change the life of these individuals.
Seppi, K., Ray Chaudhuri, K., Coelho, M., Fox, S. H., Katzenschlager, R., Perez Lloret, S., ... & Hametner, E. M. (2019). Update on treatments for nonmotor symptoms of Parkinson's disease—an evidence‐based medicine review. Movement Disorders, 34(2), 180-198
Deb Gulbrandson, PT, DPT is teaming up with Frank J Ciuba DPT, MS to create a new course called Osteoporosis Management: A Comprehensive Approach for Healthcare Professionals! This new course is launching remotely this July 25-26, 2020, and it emphasizes visual imagery cues which leads to enhanced performance for patients. Both course authors are trained by Sara Meeks, and have adapted her method to create this updated, evidence-based course on osteoporosis management.
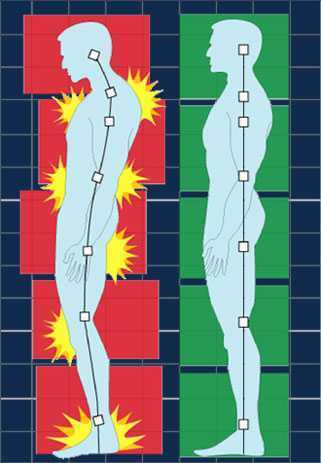
How many times have you told your patients to stand up straight and stop looking down while walking? How’d that work out? Probably not so good. At best you may have noticed a temporary correction only for the patient to return to the formerly mentioned poor posture. We know that balance is affected by alignment of our trunk and spine. 1 Everyone needs to avoid falls but it’s particularly important with osteoporosis patients due to bone fragility.
 We want our patients not only to move, but to move with optimal alignment. According to Fritz, et al 2 in the vhitepaper: “Walking Speed: The Sixth Vital Sign”, walking is a complex functional activity. Our ability to influence motor control, muscle performance, sensory and perceptual function, endurance and habitual activity level can result in a more efficient and safer gait.
We want our patients not only to move, but to move with optimal alignment. According to Fritz, et al 2 in the vhitepaper: “Walking Speed: The Sixth Vital Sign”, walking is a complex functional activity. Our ability to influence motor control, muscle performance, sensory and perceptual function, endurance and habitual activity level can result in a more efficient and safer gait.
Visual imagery cuing had been popular in the sports world for decades. By changing one or two words, physical performance has been shown to improve. 3 In a study involving standing long jump, Wu et al instructed undergraduate students to either “Jump as far as you can and think about extending your legs” (internal focus) or “Jump as far as you can and think about jumping as close to the green target as possible” (external focus). The external focus group jumped 10% farther. Lohse et al 4 and Zachry et al 5 surmised that an external focus reduces the "noise" in the motor system which affects muscular tension and optimal function.
It Starts with Posture
Before you can expect your patients to walk well, they have to stand well- stability before mobility. Assess their posture from all angles and determine where to start. One visual image may change a host of problems. A common postural fault, “slumping” is seen as forward head, increased thoracic kyphosis accompanied with either lumbar hyper or hypo lordosis. Your goal is to get the optimal alignment image that you have in your mind……. into their body.
Most people think in pictures rather than words. 6 Yet the medical industry uses words to communicate. Often we say, “Don’t slouch. Don’t look down.” Telling your patient what not to do is not helpful. Our brain hears the words, “Slouch or look down.” We don’t discern the negative. If I say to you, “Don’t think of a pink elephant,” what does your mind see? How can you not see a pink elephant?
Below are five common visual cues to improve a patient’s posture in standing and walking. These tend to follow the Pareto Principle. 20% of your cues work 80% of the time.
- “In standing, imagine a bungee cord running from the top of your head to the ceiling. Visualize a mother cat lifting her kitten up by the scruff of the neck.”
- “When breathing, imagine an umbrella inside your ribcage, opening up upon inhale, and closing on exhale. Breathe in all directions including into the back of your lungs as if you were filling up the sails of a sailboat.”
- “When walking, widen your collarbones as if they were arrows, shooting off the tips of your shoulders. Imagine your head is a floating balloon, gliding along above your shoulders.”
- “Pretend you are the King (or Queen) of England as you walk among your subjects. “
- “Slide your shoulder blades down toward your opposite hip pockets.”
Choose a cue and instruct your patient. Observe changes in posture, alignment, efficiency of movement, or length of step during gait. Ask your patient for feedback. “What did you notice?” Certain cues resonate more than others. Give them variety and options. The best cues are the ones they create themselves. When a patient says, “You mean like………..?” you know it’s a great cue for them. They have an intuitive understanding and relate to it which translates into their body. A patient’s response to the bungee cord cue was, “You mean like a Christmas ornament hanging from the tree?” My response? Absolutely!
While some visual cues may seem too flowery or not “medical” enough, the research is solid the impact powerful. Plus your patients love it! Visual cues are sticky. They help remind us when we’re out in the real world. Isn’t that the ultimate goal – helping patients become independent in their pursuit of health and safety?
1. Shiro Imagam, et all. Influence of spinal sagittal alignment, body balance, muscle strength, and physical ability on falling of middle-aged and elderly males. Eur Spine J. 2013 Jun;
2. Fritz S. et al White Paper: “Walking Speed: The Sixth Vital Sign” J Geriatr Phys Ther. 2009
3. Wu, et al Effect of Attentional Focus Strategies on Peak Force and Performance in the Standing Long Jump. Joun of Strength and Conditioning Research 2012
4. Lohse and Sherwood Defining the Focus of Attention: Effects of Attention on Perceived Exertion and Fatigue
5. Zachry, T et al. Increased Movement Accuracy and Reduced EMG Activity as a Result of Adopting an External Focus of Attention. Brain Research Bulletin Oct 2005
6. Dynamic Alignment Through Imagery. Franklin, Eric. Second Edition, 2012

Kate Bailey, PT, DPT, MS, E-RYT 500, YACEP, Y4C, CPI joins the Herman & Wallace faculty with her new course on Restorative Yoga for Physical Therapists, which is launching in remote format this June 6-7, 2020. Kate brings over 15 years of teaching movement experience to her physical therapy practice with specialities in Pilates and yoga with a focus on alignment and embodiment. Kate’s pilates background was unusual as it followed a multi-lineage price apprenticeship model that included study of complementary movement methodologies such as the Franklin Method, Feldenkrais and Gyrotonics®. Building on her Pilates teaching experience, Kate began an in depth study of yoga, training with renown teachers of the vinyasa and Iyengar traditions. She held a private practice teaching movement prior to transitioning into physical therapy and relocating to Seattle.
 Yoga is a common term in our current society. We can find it in a variety of settings from dedicated studios, gyms, inside corporations, online, on Zoom, at home, and on retreat. The basic structure of a typical yoga class is a number of flowing or non flowing postures, some requiring balance, some requiring going upside down, and many requiring significant mobility to achieve a certain shape. At the end of these classes is a pose called savasana, corpse pose (or sometimes translated for comfort as final resting pose). In this pose, which is often a treat for students after working through class, students lie on the ground, eyes closed, possibly supported by props, and rest. It is perhaps the only other time in the day when that person is instructed to lie on the floor in between sleep cycles.
Yoga is a common term in our current society. We can find it in a variety of settings from dedicated studios, gyms, inside corporations, online, on Zoom, at home, and on retreat. The basic structure of a typical yoga class is a number of flowing or non flowing postures, some requiring balance, some requiring going upside down, and many requiring significant mobility to achieve a certain shape. At the end of these classes is a pose called savasana, corpse pose (or sometimes translated for comfort as final resting pose). In this pose, which is often a treat for students after working through class, students lie on the ground, eyes closed, possibly supported by props, and rest. It is perhaps the only other time in the day when that person is instructed to lie on the floor in between sleep cycles.
Savasana is one of many restorative yoga postures. In the work created and popularized by Judith Hanson Lasater, PT, PhD1, restorative yoga has taken a turn away from the active physical postures, breath manipulations and meditations that are commonplace in how we think of yoga. She has focused on rest and the need for rest in our current climate of productivity, poor self-care, and difficulty managing stress and pain.
In a dedicated restorative yoga class (not a fusion of exercise then rest, or stretch then rest… which are really lovely and have their own benefits), a student comes to class, gathers a number of props, and is instructed through 3 to 5 postures, all held for long durations to complete an hour or longer class. Consider what it would look like to do 3 things over one hour with the intent of resting. It is quite counter-culture. Students have various experiences to this type of practice, but overtime many begin to feel the need for rest (or restorative practice) in a similar way that one feels thirsty or hungry.
We know the benefits of rest: being able to access the ventral vagal aspect of the parasympathetic nervous system is what Dr. Stephen Porges2 suggests supports health, growth and restoration. There is impact on the ventral vagal complex in the brainstem that regulates the heart, the muscles of the face and head, as well as the tone of the airway. To heal, we need access this pathway. To manage stress, we need to access this pathway. To be able to choose our actions rather than be reactionary, we need to access this pathway. Restorative yoga is an accessible method that may be a new tool in a patient’s tool box to help manage their nervous systems.
1. Relax and Renew: Restful Yoga for Stressful Times by Judith Hanson Lasater PT, PhD
2. Polyvagal Theory by Stephen W Porges PhD
Last week- on May 6 amid a pandemic- the Department of Education released changes to Title IX. Title IX is a 1972 Civil Rights Act that bans sexual discrimination within the educational system. Sadly, the new provisions within the 2,033 page document include the following changes:
- Narrows the definition of sexual harassment
- Reduces options to survivors of sexual assault, dating violence and stalking
- Reduces liability of colleges and universities
- Reduces mandated reporting of sexual violence
- Deregulates federal guidelines to protect sexual violence survivors
- Changes the ‘standard of proof’ from ‘preponderance’ to ‘clear and convincing’
- Bolsters protections for perpetrators
- Allows for live hearings and cross examinations of the assault survivor
- Only investigates if assault reported to ‘certain people’
23% of undergraduates and 11% of graduate students report having experienced sexual violence, AND we know survivors under-report assaults. We talk extensively about medical and legal considerations for sexual violence survivors in my "Empowering the Sexual Assault Survivor" course. Participants who took my course will need to know those protections we discussed just a few days ago are slated to be rolled back. Today, in my remote course "Trauma Informed Care", we lay the physiological and neurobiological framework for empowering the sexual assault survivor. Following that, in addition to how to continue empowering for survivors, we elaborated on the legal changes listed above.
Outrageously, these Title IX deregulating provisions are to go into effect August 14, 2020 while schools are struggling to keep students safe amid coronavirus pandemic. Again, let us look at these percentages (23% of undergraduates, and 11% of graduate students) and think about who needs safety and protection.
Schools do have choice in whether they roll back their protections to survivors of sexual violence. If you're looking for ways to help, you may want to reach out to your alma mater and ask what changes they are planning to make in the context of this new deregulation and disempowerment of Title IX protections. Maybe contact your local sexual assault coalition and see how you can become involved. You could also contact your legislature and/or leave comment on www.regulations.gov (search title IX and education).Empower yourself so that you can empower others! As a physical therapist specialized in pelvic rehabilitation, empowering survivors of sexual violence happens every day in my practice. I hope you feel empowered, supported and successful in doing this challenging work too!

It’s OK to be feeling (insert feeling) right now. (maybe: sad, fearful, angry, denial, numb, anxious, avoidant, bored?)
 It’s OK to acknowledge those feelings.
It’s OK to acknowledge those feelings.
It’s also OK to create a plan and direction about what we may do about our feelings, thoughts, and actions.
We can change how we think, what we do and ultimately how we feel.
Breathe. Place a hand on your chest and a hand on your abdomen. Practice inhaling long and deep as if you were pouring the air into your body- first filling the lower hand and then filling the top hand. Pause for a moment when you feel your canister is full and then exhale slowly (top to bottom or bottom to top- either works fine). I prefer breathing through my nose for inhale and exhale but know if you are congested, mouth breathing is fine or you can inhale through the nose and exhale through the mouth- find what works for you. Work on increasing the number counted (silently in your mind) while you inhale, pause briefly and then exhale- making that number count on exhale the same or even longer. Make it a game to see how long and deep your breath can become. Reduce intensity if feeling lightheaded.
Focus on your breath and feel calmness. Return to this breathing whenever you can.
Body Scan/Progressive Relaxation. Take a moment and scan your body for pain or tension. You can start at the top of your body or where your feet are grounded to floor. Notice your body and allow it to be, without judgement. Then starting from the top of your body or the bottom, contract your muscles systematically and then relax. Or focus on the muscle group and allow the muscles to relax and slacken. Maybe send your long, deep breath to each area? Maybe think of color washing each area? Make your scan personal and positive for you. Check-in to your body without judgement and send gratefulness for the work your amazing body does.
Stand Big. Find a wall and place your backside onto it. Pretend there is a string at the crown of your head and imagine your head being pulled up towards the ceiling. Lift your chest as you are standing tall and use your slow, steady, deep breathing to create bigness and calmness. Relax your shoulders. Maybe place the back of your hands onto wall and feel the opening of your chest. Once you have practiced this posture, you can refer to this posture during your day. Stand big, breathe big, be big.
Intentionally SCHEDULE into your life what you love. Schedule time listening to your favorite music. Maybe take up playing an instrument? Practice singing in the shower or car. Set a timer and dance fervently. Create time to draw or paint or write. Make a recipe. Get frozen berries and make smoothies. Maybe add frozen spinach to your smoothie?
Pick up a book. Play a game, cards or even solitaire. Practice Sudoku. Take a bath or shower. Go for a long walk while keeping your distance from others. Find a workout you can do at home that makes you feel powerful. Whatever you love, turn it into a scheduled ritual. Make one small goal and work towards it. Focus on what we can do instead of what we cannot. Find some activity and fulfill a passion just for you. Make sleep a priority and know if you have a bad night, that the next night you will likely sleep better. Perhaps create a sleeping ritual? Call others and ask what they are doing for themselves? Remember to forgive yourself and to feel or express the feelings that are within you. We are all going through this together. Make you a priority and schedule yourself some HAPPY.
Lastly- try to limit the news, your phone and the frig. All of these can create negative feelings that do not fulfill us.
Breathe. Find love in positive activities. Be brave. Be grateful. Forgive.
We are all in this together.
Lauren Mansell DPT, CLT, PRPC is the author and instructor of the Trauma Awareness for the Pelvic Therapist course. She is also offering several courses via Zoom video conference during the Covid-19 pandemic, which can be found on our Remote Learning Opportunities page. Prior to becoming a physical therapist, Lauren counseled suicidal and homicidal SES at-risk youth who had survived sexual violence. Lauren was certified as a medical and legal advocate for sexual assault survivors in 1999 and has advocated for over 130 sexual assault survivors of all ages in the ED. Lauren's physical therapy specialty certifications include Certified Lymphedema Therapist (CLT), Pelvic Rehabilitation Professional Certificate (PRPC) and Certified Yoga Therapist (CYT). She is a board member of Chicagoland Pelvic Floor Research Consortium, American Physical Therapy Association Section of Women's Health and Section of Oncology.
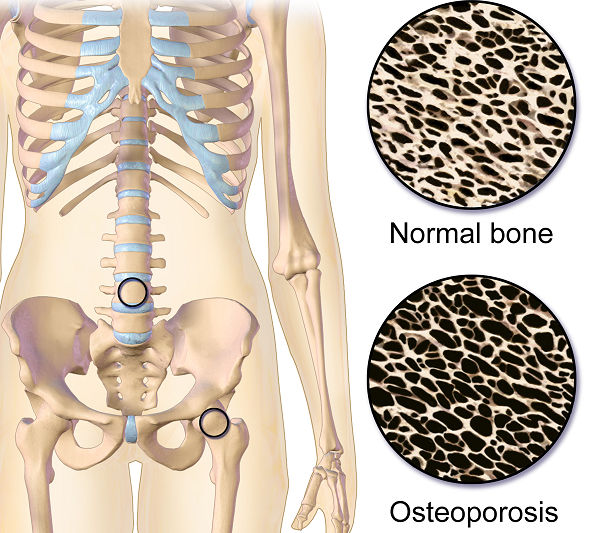
Osteoporosis or low bone mass is much more common than most people realize. Approximately 1 in 2 women over the age of 50 will suffer a fragility fracture in their lifetime. A fragility fracture is identified as a fracture due to a fall from a standing height. According to the US Census Bureau there are 72 million baby boomers (age 51-72) in 2019. Currently over 10 million Americans have osteoporosis and 44 million have low bone mass.
Many myths abound regarding osteoporosis. Answer these 5 questions below to test your Osteoporosis IQ. 1
1. “Men don’t get osteoporosis.”
 Fact: In addition to the statistic above regarding the incidence of fractures in women, up to 1 in 4 men over the age of 50 will suffer a fragility fracture.
Fact: In addition to the statistic above regarding the incidence of fractures in women, up to 1 in 4 men over the age of 50 will suffer a fragility fracture.
2. “Osteoporosis is a natural part of aging.”
Fact: Although we do lose bone density as we age, osteopenia or osteoporosis is a much more significant loss than seen in normal aging. DXA (dual energy x-ray absorptiometry) is the gold standard for measuring bone density and the test shows whether an individual’s numbers fall into the normal, osteopenia, or osteoporosis range based on his or her age.
3. “I don’t need to worry about osteoporosis until I’m older.”
Fact: Osteoporosis has been called a “pediatric condition which manifests itself in old age.” Up until the age of 30 we build bone faster than it breaks down. This includes the growth phase of infants and adolescents and is also the time to build as much bone density as possible. By the age of 30, called our Peak Bone Mass, we have accumulated as much bone density as we will ever have. Proper nutrition, osteoporosis specific exercises, and good body mechanics in our formative years can all play a role in reducing the effects of low bone mass later on.
4. “I exercise regularly (including sit ups and crunches for my core). I would know if I had a fracture.”
Fact: Two myths here. Flexion based exercises such as sit-ups, crunches, and toe touches are contraindicated for osteoporosis. A landmark study done by Dr. Sinaki from Mayo clinic showed women with osteoporosis had an 89% re-fracture rate after performing flexion based exercises. 2
Fact: Secondly, only 30% of vertebral compression fractures (VCF) are symptomatic meaning many individuals fracture without knowing it. This can lead to a fracture cascade as individuals continue performing movements and exercises that are contraindicated.
5. “Tests for osteoporosis are painful and expose you to a lot of radiation.”
Fact: The DXA is a simple and painless test which lasts 5-10 minutes. You lay on your back and the machine scans over you with an open arm- no enclosed spaces. There is very little radiation. Your exposure is 10-15 times more when flying from New York to San Francisco.
How did you do? Feel free to share these myths with your patients, many of whom may have osteoporosis in addition to the primary diagnosis for which they are being treated. To learn more about treating patients with low bone density/osteoporosis, consider attending a Meeks Method for Osteoporosis course!
1. www.nof.org
2. https://www.ncbi.nlm.nih.gov/pubmed/6487063
3. https://www.aafp.org/afp/2016/0701/p44.html
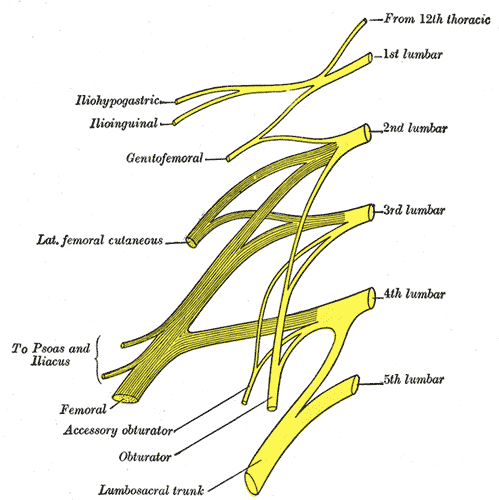
The lumbar sacral nerve plexus can be divided into the direction the nerves travel, either anterior or posterior. This post will focus on anterior hip nerves. I remember writing about the brachial plexus over and over in physical therapy school, but only a few times for the lumbosacral plexus. Patients frequently report anterior hip and pubic pain and can often have signs and symptoms of nerve entrapment. This article orients the reader to links between signs and symptoms and examination to help appropriately diagnosis specific nerves in the athletic population.
 The obturator, femoral and lateral femoral cutaneous are more commonly entrapped in sports injuries. Although the three nerves that travel together through the inguinal canal (ilioinguinal, iliohypogastric, and genitofemoral) are less common, however surgery can create nerve entrapment sequelae.
The obturator, femoral and lateral femoral cutaneous are more commonly entrapped in sports injuries. Although the three nerves that travel together through the inguinal canal (ilioinguinal, iliohypogastric, and genitofemoral) are less common, however surgery can create nerve entrapment sequelae.
There are a few places where the obturator nerve can become squished. Typically, as it leaves the obturator canal which presents at medial thigh pain, and then again in the fascia of the adductors which presents as pain with abduction. The challenge is to differentiate between the nerve and adductor strain. Obturator nerve entrapment will test positive with passive hip abduction and extension, but negative resisted hip adduction.
The femoral nerve can become entrapped in a kind of compartment syndrome as it goes between the psoas and iliacus. This can lead to compression to the neurovascular bundle with resultant swelling, edema, and ischemia. Signs of femoral nerve compression include anterior thigh numbness and paresthesias. Occasionally, this can also include the saphenous nerve with symptoms continuing along medial knee to foot. Femoral nerve entrapment can create quadricep muscle weakness and atrophy, with diminished or absent patella tendon reflexes. Symptoms are reproduced with hip extension and knee flexion thereby elongating the femoral nerve.
The lateral femoral cutaneous (LFC) nerve is sensory. Diagnosed as meralgia paresthetica, the LFC nerve is typically entrapped where it penetrates under the inguinal ligament just medial to the anterior superior iliac spine (ASIS). Symptoms include numbness, tingling, hypersensitivity to touch, burning along outer thigh along the iliotibial band. The LFC nerve can often be compressed by wearing heavy belts (scuba divers, construction belts, etc). Special tests that indicate LFC are pelvic compression in side lying with involved side up to slack the inguinal ligament and Tinels sign.
Anterior hip pain is fairly common in pelvic floor patients. Differential diagnosis and treatment of these anterior nerves can allow patients to return to full daily function. To learn manual assessment and treatment techhniques for the lumbar nerves, consider attending Lumbar Nerve Manual Assessment and Treatment.
Martin R, Martin HD, Kivlan BR. Nerve Entrapment In The Hip Region: Current Concepts Review. Int J Sports Phys Ther. 2017 Dec;12(7):1163-1173.

I recently assisted at a Pelvic Floor Level 2B course which has been updated with recent research, new sections, and less repetition from Pelvic Floor Level 1. In the course they mentioned this article which sparked a lively discussion and I had to learn more. It is rare to see a study with a large number of participants in pelvic health and especially with a vaginismus diagnosis.
Vaginismus is defined as a genito-pelvic pain/penetration disorder along with dyspareunia under the DSM-5 (Diagnostic and Statistical Manual of Mental Disorders; Fifth Edition) in which penetration is often impossible due to pain and fear. Vaginismus is both a physical and psychological disorder as it exhibits both muscle spasms and fear/anxiety of penetration. Symptoms vary by severity. Common presentation is an inability or discomfort to insert/remove a tampon, pain with penetration, and complaints of “hitting a wall” in attempted penetration; and inability to participate in gynecological exams.
 The authors of this study evaluated the severity of vaginismus. The penetrative history was used in addition to presentation at pelvic exam, and then given a level. There are 2 grading systems, Lamont and Pacik, that indicate the level of fear and anxiety about being touched. They found that those with severe vaginismus were Lamont levels 3 and 4, and Pacik level 5. For example, a Pacik Level 5 includes Lamont grade 4 “generalized retreat: buttocks lift up; thighs close, patient retreats” plus a visceral reaction such as “palpitations, hyperventilation, sweating, severe trembling, uncontrollable shaking, screaming, hysteria, wanting to jump off the table, a feeling of going unconscious, nausea, vomiting and even a desire to attack the doctor”.
The authors of this study evaluated the severity of vaginismus. The penetrative history was used in addition to presentation at pelvic exam, and then given a level. There are 2 grading systems, Lamont and Pacik, that indicate the level of fear and anxiety about being touched. They found that those with severe vaginismus were Lamont levels 3 and 4, and Pacik level 5. For example, a Pacik Level 5 includes Lamont grade 4 “generalized retreat: buttocks lift up; thighs close, patient retreats” plus a visceral reaction such as “palpitations, hyperventilation, sweating, severe trembling, uncontrollable shaking, screaming, hysteria, wanting to jump off the table, a feeling of going unconscious, nausea, vomiting and even a desire to attack the doctor”.
241 patients participated in this study, with a mean duration of 7.8 years. 70% of participants were a Lamont level 4 or Pacik level 5 at baseline. The authors looked at previous treatments tried and coping strategies; 74% had tried lube, 73% had tried dilators, 50% had tried Kegels, 28% had tried physical therapy, 3% had tried a surgical vestibulectomy. The full table 2 is in the article. Most participants had a mean of at least 4 failed treatments.
The aim was to help these women to achieve pain free intercourse after treatment. In order to tolerate the treatment, many were sedated with midazolam before the Q-tip test, and more sedation given as needed. The treatment lasted for about 30 minutes and consisted of:
- Q-tip test with as minimal sedation as possible to rule out vulvodynia and provoked vestibulodynia
- Digital exam of tolerance in order to assess the level of spasm in introitus. Graded 0 (no spasm) to 4 (severe spasm where digital insertion was difficult)
- Botox 50 U injections to right and left submucosal space near the bulbospongiosus muscle administered with a pediatric speculum placed. Additional Botox was injected submucosally into levator ani muscles if also in spasm/tight
- Injections 0.25% bupivacaine (a numbing agent) 1 mL increments along right and left lateral vaginal walls (9 mL per side) from cervix to introitus
- Progressive dilation; circumference 3 inches (#4), 4 inches (#5), 5 inches (#6)
- Reassessed with digital examination
- Re-insert #5 or #6 dilator and patient was awakened and taken to recovery
If the patient consented, her partner could be present during the procedure and was allowed to palpate the level of spasm with gloved digit and was educated on dilator insertion. The authors noted that many partners had a ‘profound’ experience.
A nurse worked with the couple for about two hours in the recovery room to help them be more comfortable moving the dilator in and out with minimal-to-no pain as the numbing agent lasts 6-8 hours. Three participants were treated each time and consented to meet each other. Patients were discharged with #4 dilator in place and asked to keep in until the next day. They were given Ibuprofen and sleeping aids as needed.
Day 1
Participants return with partners and progress up to larger sizes (#5 and #6). They participate in group counseling with the primary researcher Dr. Pacik. This lasted about 5 hours; and consisted of education of dilator progression, returning to intercourse and lubricants. If participants wished to have private counseling instead that was granted. Many exchanged contact information. They were encouraged to continue seeing their healthcare clinicians as indicated; sex therapists, physical therapists, psychologists.
Dilator Progression
Month 1
- 2 hours of dilator per day. Either in 1 sitting or 1 hour of dilator work x2 per day
- Progress to bigger sizes until #5 or #6 is comfortable
Month 2
- 1 hour of dilator use per day and continue toward larger sizes
Month 3
- 15-30 minutes of dilator use per day
Months 4-12
- 10-15 minutes of dilator use per day or every other day
During the counseling session post-procedure, the recommendations for returning to intercourse included:
- Delaying intercourse until #5 dilator was able to be easily inserted
- It is helpful to do 1 hour of dilator work before attempting intercourse for the first time
- If partner’s penis is larger progress to larger dilators (#7 - 6 inch circumference or #8 7 inch circumference)
- Goal of the first few attempts is to insert tip of dilator only
- Once tip can be inserted easily then progress to full penetration; restrain from thrusting
- Try “spooning position” if ‘leg lock’ occurs
- Try different positions with dilator work and intercourse to see what works best
71% of participants achieved pain-free coitus 5 weeks after the procedure. 2.5% could not achieve coitus within one-year period although they could use #5 or #6 dilators. The participants were given a validated outcome tool, the Female Sexual Function Index (FSFI), before and after the procedure and at 1-month, 3-months, 6-months, and 1-year; with significant improvement at each interval. The patients were followed for one year, and often remained in contact with the authors for much longer ranging from 16-months to 9-years.
The authors propose that use of dilators at the time of botox and post procedure counseling and support help participants ‘break through’, whereas previous treatment may not be as multidimensional and limit efficacy. Botox lasts 2-4 months and allowed for dilation progression.
Initially after reading this article the treatment seemed a little drastic to me, but then I considered the women with this level of vaginismus are often not coming into my clinic. They may need this level of structure, consistently, and multidimensional treatment as half measures have failed them. I am so glad they were persistent and found the help they needed.
Pacik, P., Geletta, S. Vaginismus Treatment: Clinical Trials Follow Up 241 Patients. Sex Med 2017;5:e114-e123

The female sexual response cycle is more than physical stimulation. As pelvic therapists, we frequently find ourselves treating pelvic pain that has interrupted a woman’s ability to enjoy her sexuality and sensuality. As physical therapists, we focus on the physical limitations and pain generators as a way of helping patients overcome their functional limitations. However, many of us find that once many of the physical symptoms have cleared with pelvic floor and fascial stretching, our patients are still apprehensive to engage physically, or they are not able to derive pleasure. There is clearly a gap that needs to be bridged that goes beyond pain.
 Last year I taught my class, Lumbar Nerve Manual Assessment and Treatment. I was honored and astounded to have Dee Hartmann, PT in my class. For those of you who do not know Dee, she has been a champion of our field for a long time, and she has been instrumental in elevating physical therapy as a first line of treatment in pelvic pain through her work, international leadership, and representation in multiple organizations, including APTA SOWH, ISSVD, IPPS, NVA, ISSWSH, and as an editor for the Journal of Sexual Medicine.
Last year I taught my class, Lumbar Nerve Manual Assessment and Treatment. I was honored and astounded to have Dee Hartmann, PT in my class. For those of you who do not know Dee, she has been a champion of our field for a long time, and she has been instrumental in elevating physical therapy as a first line of treatment in pelvic pain through her work, international leadership, and representation in multiple organizations, including APTA SOWH, ISSVD, IPPS, NVA, ISSWSH, and as an editor for the Journal of Sexual Medicine.
In this manual nerve class, I was teaching how to treat the path of the genitofemoral nerve, which affects the peri-clitoral tissues and sensation. We also covered manual therapy approaches to decrease restriction in the clitoral complex and improve the blood flow response in this region. Dee was fascinated and looped me into what she had been working on for the past several years. She has been working as part of a company called Vulvalove with her partner, sex therapist, Elizabeth Wood on studying and teaching women how to recapture their sensuality. Immediately, we wanted to combine forces in some way to present a way to approach these issues. So, when Dee invited me to present with Elizabeth and her at the Combined Sections Meeting of the American Physical Therapy Association (CSM) this year, I was humbled and excited to jump on board.
With improved tissue mobility in the clitoral and vaginal area, blood flow is able to improve through any previously restricted tissues. With any manual therapy or soft tissue work, it is expected that cutaneous circulation of blood and lymph will alter. In studies, a measure of this blood flow, VPA (Vaginal Pulse Amplitude) is higher in the arousal than the non-arousal state in women.4 “The first measurable sign of sexual arousal is an increase in the blood flow. This creates the engorged condition, elevates the luminal oxygen tension and stimulates the production of surface vaginal fluid by increased plasma”.5 Manual therapy can likely affect this.1,2. During our CSM talk, I will discuss the neurovascular anatomy and will have a brief video of manual techniques to enhance these pathways in my portion of the presentation.
In the 19th century, female orgasm and sensuality was believed to be more vaginal, but as the 20th century unfolded, understanding of the clitoral tissues improved. More recent research reveals the origin of female pleasure is more complex, involving the clitoris, vulva, vagina, and uterus.3 However, female response is more complicated than just anatomy below the waist.
Heart Rate Variability (HRV) is a measure of autonomic nervous system health and the ability to flux between sympathetic and parasympathetic states. Autogenic training and meditation or mindfulness have been shown in multiple studies to improve HRV. A study by Stanton in 2017 demonstrated that even one session of autogenic training can increase HRV and VPA (Vaginal Pulse Amplitude, a measure of arousal). In our talk at CSM, Dee will cover the role of autogenics and how to specifically and practically use our autonomic state to influence our perception and feeling of pleasure. Dee will also cover extensive clitoral anatomy to have a better understanding of how this intricate complex functions and is structured in women.
Elizabeth Wood, a former sex therapist who is now a sex educator, will then present on the arousal cycle and what can be done physiologically to prepare the arousal network for climax. Elizabeth will help us to better define and understand the roles of arousal, calibration, and exploring sensuality, including exercises to help a patient have a more fulfilling experience once the physical pain is resolved. As Elizabeth says, “Knowledge is an antidote to shame and an invitation to pleasure”.
If you will be at CSM, please come join us at the opening session, Thursday February 13 from 8am-10am (PH2540), “Now That The Pain Is Gone, Where’s the Pleasure”.
If you can’t make it to CSM, I hope to see you at one of my nerve classes, “Lumbar Nerve Manual Therapy and Assessment” this year in Madison, WI April 24-26 or Seattle, WA October 16-18 to further explore manual therapies to improve sensation and neural feedback loops and to continue this conversation!
1. Portillo-Soto, A., Eberman, L. E., Demchak, T. J., & Peebles, C. (2014). Comparison of blood flow changes with soft tissue mobilization and massage therapy. The Journal of Alternative and Complementary Medicine, 20(12), 932-936.
2. Ramos-González, E., Moreno-Lorenzo, C., Matarán-Peñarrocha, G. A., Guisado-Barrilao, R., Aguilar-Ferrándiz, M. E., & Castro-Sánchez, A. M. (2012). Comparative study on the effectiveness of myofascial release manual therapy and physical therapy for venous insufficiency in postmenopausal women. Complementary therapies in medicine, 20(5), 291-298.
3. Colson, M. H. (2010). Female orgasm: Myths, facts and controversies. Sexologies, 19(1), 8-14.
4. Rogers, G. S., Van de Castle, R. L., Evans, W. S., & Critelli, J. W. (1985). Vaginal pulse amplitude response patterns during erotic conditions and sleep. Archives of sexual behavior, 14(4), 327-342.
5. Stanton, A., & Meston, C. (2017). A single session of autogenic training increases acute subjective and physiological sexual arousal in sexually functional women. Journal of sex & marital therapy, 43(7), 601-617.

Lila Abbate PT, DPT, OCS, WCS, PRPC is the creator and instructor of Bowel Pathology Function & Dysfunction and the Pelvic Floor, a course which instructs in comprehensive evaluation and treatment techniques for bowel pathologies and dysfunctions, including fecal incontinence, chronic constipation, and the relationship between constipation and rectal and/or abdominal pain. Join Dr. Abbate in one of five events taking place in 2020!
Bowel dysfunction can be very rewarding to treat. Most pelvic health physical therapists are nervous about diving into bowel treatment. When I was training with my mentor, Elise Stettner, PT she used to remind me that “any PT can treat urinary symptoms. The patients who are really suffering are those bowel dysfunctions.” That statement really stuck with me and mentoring with her and treating those patients created a passion for treating patients who suffer from bowel dysfunction.
 Within the term bowel dysfunction, fecal urgency, is a common symptom and is under-researched. In 2019, Similis, et al published A Systemic Review and Network Meta-Analysis Comparing Treatments for Faecal Incontinence, doesn’t even mention physical therapy and pelvic floor muscle rehabilitation as an intervention for fecal incontinence and fecal urgency treatment.
Within the term bowel dysfunction, fecal urgency, is a common symptom and is under-researched. In 2019, Similis, et al published A Systemic Review and Network Meta-Analysis Comparing Treatments for Faecal Incontinence, doesn’t even mention physical therapy and pelvic floor muscle rehabilitation as an intervention for fecal incontinence and fecal urgency treatment.
Anecdotally, I have a lot of pelvic health patients and even generalized orthopedic patients who report that having bowel urgency is a more apparent symptom in their life after having a back or hip surgery. What started as a once-in-a-while problem, fecal urgency has crept up and become the new normal in their lives. They have subliminally re-routed their day to accommodate their bowel movements in order avoid incidences and accidents whether its waiting to eat breakfast until they get to work, waiting to drink a favorite drink until they are near a toilet or taking supplements before bed to empty their bowels before they start their day in order to avoid accidents during their day. Learning to treat bowel urgency can tremendously help patients regain control and abolish their symptoms.
Bowel urgency has many parallels to urinary urgency. The colon is giving the signal too soon, potentially at an inappropriate time, and the muscles need to be strong enough to hold the urge of defecation back in order to postpone. The failure occurs when one part of the continence mechanism fails. Bowel Pathology Function & Dysfunction and the Pelvic Floor course helps you to learn how to treat and guide your patients and conquer all types of bowel dysfunction.
Similis et al, A systematic review and network meta-analysis comparing treatments for faecal incontinence. Int J Surg. 2019 Jun;66:37-47. doi: 10.1016/j.ijsu.2019.04.007. Epub 2019 Apr 22.
All Upcoming Continuing Education Courses

Mobilization of the Myofascial Layer Satellite Lab Course - Novato CA - April 4 - 6 2025
Apr 4 2025 - Apr 6 2025

Mobilization of the Myofascial Layer Satellite Lab Course - Self-Hosted - April 4 - 6 2025
Apr 4 2025 - Apr 6 2025

Mobilization of the Myofascial Layer Satellite Lab Course - Torrance CA - April 4 - 6 2025
Apr 4 2025 - Apr 6 2025

Mobilization of the Myofascial Layer Satellite Lab Course - Medford OR - April 4 - 6 2025
Apr 4 2025 - Apr 6 2025

Mobilization of the Myofascial Layer Satellite Lab Course - Milwaukee WI - April 4 - 6 2025
Apr 4 2025 - Apr 6 2025

Mobilization of the Myofascial Layer Satellite Lab Course - Danville IN - April 4 - 6 2025
Apr 4 2025 - Apr 6 2025

Pharmacologic Considerations for the Pelvic Health Provider - Remote Course - April 5 2025
Apr 5 2025

Pelvic Function Level 1 - Satellite - Tucson AZ - April 5 - 6 2025 - SOLD OUT
Apr 5 2025 - Apr 6 2025

Pelvic Function Level 1 - Satellite - Seattle WA - April 5 - 6 2025 - SOLD OUT
Apr 5 2025 - Apr 6 2025

Pelvic Function Level 1 - Satellite - Newberg OR - April 5 - 6 2025 - SOLD OUT
Apr 5 2025 - Apr 6 2025

Pelvic Function Level 1 - Satellite - Los Angeles CA - April 5 - 6 2025 - SOLD OUT
Apr 5 2025 - Apr 6 2025

Pelvic Function Level 1 - Satellite - Owensboro KY - April 5 - 6 2025 - SOLD OUT
Apr 5 2025 - Apr 6 2025



Pelvic Function Level 1 - Satellite - Charlotte NC - April 5 - 6 2025 - SOLD OUT
Apr 5 2025 - Apr 6 2025

Rehabilitative Ultrasound Imaging Pelvic Health Satellite Lab Course - Self-Hosted - April 11 - 13 2025
Apr 11 2025 - Apr 13 2025


Pelvic Function Level 1 - In-Person - Tacoma WA - April 12 - 13 2025 - SOLD OUT
Apr 12 2025 - apr 13 2025
Pelvic Function Level 2B - Satellite - Torrance CA - April 12 - 13 2025 - SOLD OUT
Apr 12 2025 - Apr 13 2025


Rehabilitative Ultrasound: Orthopedic Topics Satellite Lab Course - Self-Hosted - April 12 - 13 2025
Apr 12 2025 - Apr 13 2025

Pelvic Function Level 2B - In-Person - Philadelphia PA - April 12 - 13 2025
Apr 12 2025 - Apr 13 2025





Parkinson Disease and Pelvic Rehabilitation - Remote Course - April 25 - 26 2025
Apr 25 2025 - Apr 26 2025

Pelvic Function Level 1 - Satellite - New York NY - April 26 - 27 2025 - SOLD OUT
Apr 26 2025 - Apr 27 2025

Menopause Transitions and Pelvic Rehab - Remote Course - April 26 - 27 2025
Apr 26 2025 - Apr 27 2025



Pediatrics Level 1 - Treatment of Bowel and Bladder Disorders - Remote Course - April 26 - 27 2025
Apr 26 2025 - Apr 27 2025



Pelvic Function Level 1 - Satellite - Colorado Springs CO - April 26 - 27 2025 - SOLD OUT
Apr 26 2025 - Apr 27 2025




